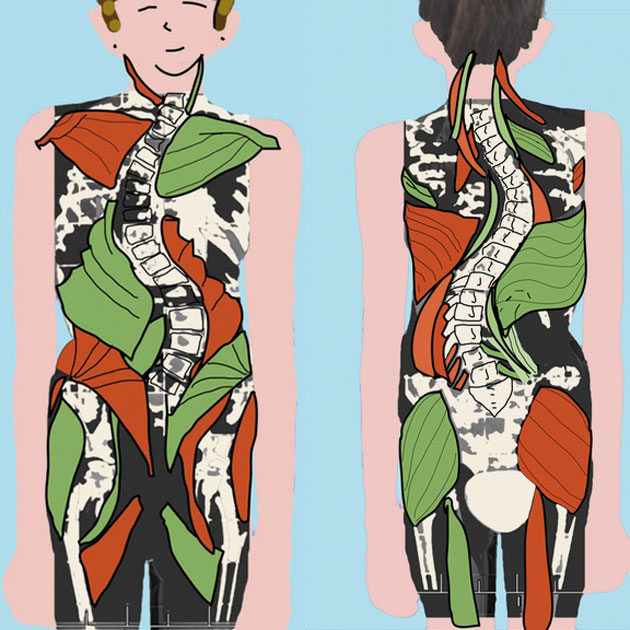
Scoliosis is characterized by asymmetrical tensions in the muscle and fascia system of the entire body. These cause the body to slowly twist and contract over the course of months and years. This is how the well-known S-shape of the spine develops. This twisting causes further symptoms such as pelvic obliquity, unevenly high shoulders, tension and headaches up to a reduced lung capacity. Scoliotic adolescents usually have no back pain.
Scoliosisis defined as a lateral curvature of the spine with simultaneous rotation of the vertebrae. The spinal column forms arches in the generally known S-shape or C-shape which compensate each other in order to maintain body weight.
Idiopathic scolioses usually develop from the age of 3 and worsen during periods of increased growth, especially between the ages of 10 and 16. The cause of idiopathic scoliosis (90%) is unknown. Functional scolioses (10 %) never reach the high degree of curvature of ideopathic scolioses. They occur, for example, as a result of vertebral fractures, operations, accidents, differences in leg length and nerve diseases.
You have probably already studied the orthodox medical findings and treatment methods for scoliosis extensively on some websites. If not, you will find a good summary of these facts in Wikipedias article about scoliosis.
How do I recognize a scoliosis?
You can recognize a scoliosis by different characteristics.
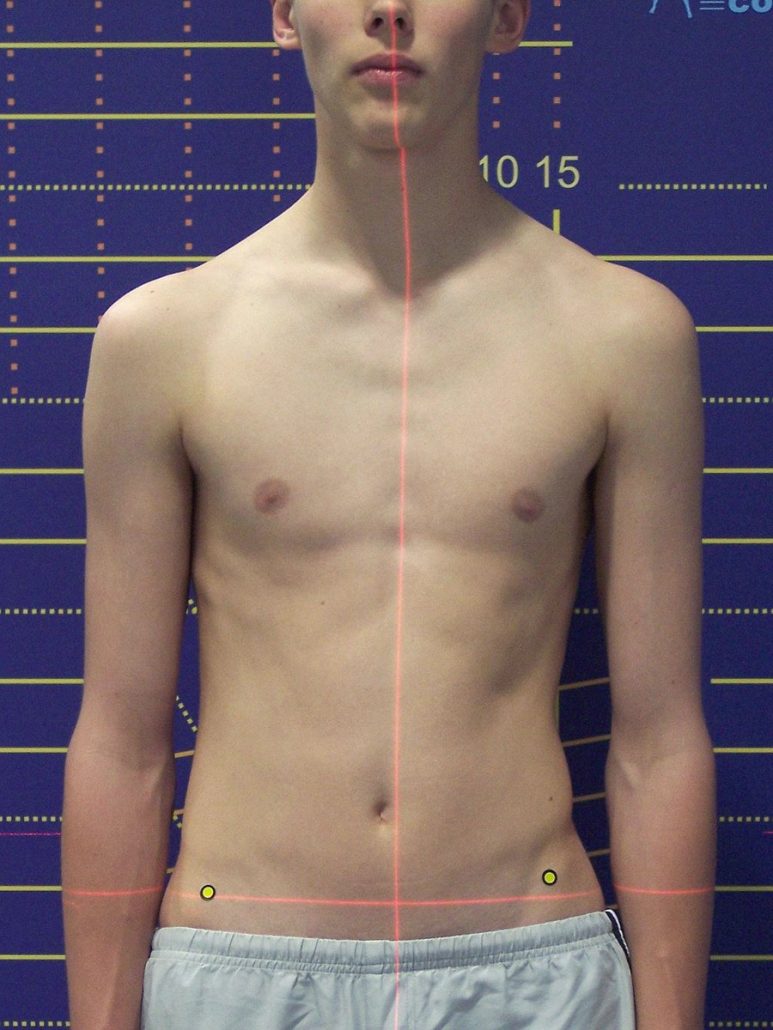
- The head does not sit in the middle over the pelvis.
- The shoulders do not have the same height.
- The tips of the shoulder blades are not at same height.
- The torso deviates from the midline. (Plumbline deviation)
- The „waist triangles“ (air space between arm and pelvis, siehe picture) have different shape and height.
- One hip is higher and more antrior and sometimes there is a leg length discrepancy.
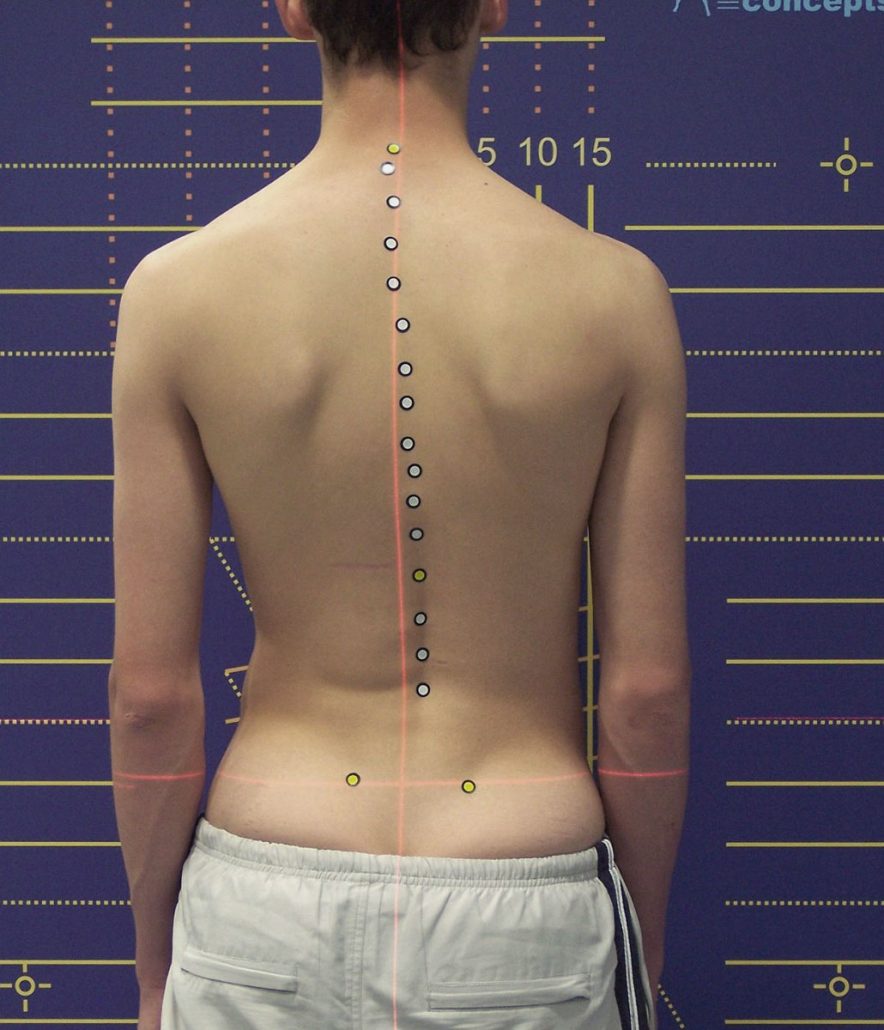
Foto: www.kid-check.de
In the Adams-Test, the patient tilts forward and lets his arms hang loosely. If you stand behind the patient and look at the bent back, you will notice a scoliosis if …
- one shoulder hangs further down, the other shoulder stands further up (incipient rib hump)
- one-sided, more pronounced lumbar muscles (the so-called lumbar bulge)
- spinal collumn has a curve
Only when you take a closer look can you see that the spinal column is often twisted by 20° to the Cobb Angle. The specialist uses an X-ray to determine the Cobb angle of the individual curvatures of the spine and the rotation of the vertebrae in the vertical plane. Important data for the prognostic course are age and in girls the first menstrual period. – As the majority of untreated scolioses worsen, early detection is of outstanding importance.
Follow-up
Only 5% of juvenile scolioses are not progressive. The remaining 95 % increase by about 1 to 5° annually until reaching the age of 10. In adolescence, i.e. after the age of 10, they increase by 5 to 10° per year during the pubertal growth spurt. Within one year the angle can shift by up to 40°. Therefore, a 3 to 6-month follow-up by a specialist is indispensable.
Radiography X-rays are necessary for the diagnosis, but they mean radiation exposure. For this reason, they should not be taken more frequently than every 6 months for children, every 12-18 months for adolescents and every 24 months for adults (2) .
Rasterstereografie = 3D spine measurement
Rasterstereografie is a light-optical measurement of the back surface. Although it is not suitable for diagnosis, it provides sufficient results for follow-up. It is state-of-the-art and is used in combination with X-rays.
Medimouse / Spinalmouse
Medimouse is a device similar to a computer mouse that is used by doctors to move along the spine. A three-dimensional image of the back line is displayed on the PC screen. The system is suitable for monitoring the progress of the therapy and its progress.
EOS 3D low-dose X-ray (Promotion Video)
The EOS x-ray generator is an alternative to classical x-rays and provides 3D x-rays with up to 80% less radiation exposure. In German-speaking countries, however, it is only used in a few clinics: at the University Hospital of Heidelberg, the Dortmund Clinic, the Friedrichsheim University Hospital, the Bad Sobernheim Clinic and the Balgrist Clinic in Zurich. You have to reckon with 250 Euro per x-ray.
Research into the cause
Progression of scoliosis
Various factors contribute to the progression of scoliosis, such as gravity itself, muscle actions, human gait, growth-induced torsion(3), and Davis’s Law(4), which states that tendons and ligaments shorten when they are not used or are too loose.
Cause of ideopathic scoliosis
As far as the state of research is concerned, slight disturbances of the sense of balance (vestibular dysfunction and nystagmus) have been frequently found in patients with scoliosis. Studies from recent years are increasingly dealing with this topic(5),(6). It is also being considered whether vestibular asymmetries could be the cause of ideopathic scoliosi (7),(8). In a metastudy the hypothesis is formulated that the origin of scoliosis lies in a slight asymmetry of the neuromuscular system(9).
I would like to ask you to consider this information when considering the following therapy options.
What are the options?
Orthodontic examination
An orthodontic examination certainly makes sense because there is a connection between scoliosis, weakness of the arch of the foot, pelvic obliquity, functional difference in leg length, asymmetries of the cervical spine and jaw asymmetries(10). Ideally, the bite plane height is tested using Professional Applied Kinesiology (PAH) techniques. The correction is then carried out by a dentist experienced in craniomandibular dysfunction (CMD).
Sensorimotor Insoles
The efficacy of sensorimotor insoles is often the subject of discussion(11), because there are large differences in craftsmanship(12) and frequent mistakes are made in advice, product selection and application. The use of sensorimotor insoles is recommended for complaints emanating from the feet. However, insoles have the disadvantage that the feet quickly get used to the stimulus and then no longer react to it. It should therefore be clear that insoles cannot be permanent for many months or even years(13). Foot strength exercises, balance exercises and manual therapy are additionally necessary so that the feet soon no longer need the insoles.
Schroth method
The Schroth method has been used successfully for many years. Severe scolioses can be treated in rehabilitation clinics such as Bad Sobernheim or Bad Salzungen. Lighter scolioses can be treated by physiotherapists with Schroth training. The method is based on a combination of physical exercises and intensive breathing. With the help of so-called rotation-angle breathing and physical stretching, the spine is untwisted or unwound. With this method considerable progress could be obtained with even the heaviest scolioses, as is proven by many studies. Christa Lehnert-Schroth’s book “Three-dimensional scoliosis treatment” provides information about this.
Voita-Methode
The Voita-Medthode is based on the activation of reflex crawling, reflex turning and reflex locomotion (reflex crawling). Prof. Václav Voita has developed the method in newborns and it is now also used in adults. Repeated triggering of the reflex-like movement leads to release and re-insertion within the blocked nervous networks between brain and spinal cord. The method has a broad spectrum of effects, for example in cerebral paresis, scoliosis or hip dysplasia. It is offered by physiotherapists with Voita training. The method should be used three to four times a day for 20 minutes by the mother on her child or partner. With babies this can be easily done, with adolescents and adults with scoliosis it seems rather difficult to integrate the method into everyday life.
Spiral Dynamics
Spiral Dynamics is a three-dimensional movement concept that is occasionally offered by physiotherapists. The principle and the exercises from spiral dynamics are used in scoliosis treatment. One tries here to dissolve the scoliotic twisting of the body with a natural counter spiral. With the movement concept you have a nice introduction to understand the functioning of your body in movement. There are no studies on the effectiveness. Spiraldynamik AG offers 3-day seminars in Zurich for scoliosis patients. With the book “Skoliose Aufrecht durch Bewegung: Die besten Übungen aus der Spiraldynamik” by Christian Larsen will get you a good introduction and at the same time you can recognize the limits of the method.
Yoga, Pilates und Gyrotonic
You can use Yoga, Pilates or Gyrotonic to accompany scoliosis therapy. However, it should be remembered that with global stretching you help the body to become more elastic, but with stretching you usually do not reach the “hot spots”, i.e. the locally highly tense parts of the body, and run the risk that the spinal column therefore evades into the scoliotic pattern, and the scoliosis thus intensifies and progresses faster (14). The methods are therefore only suitable under expert guidance as an accompaniment to manual scoliosis therapy.
Sport
Dancers, swimmers and gymnasts have a lower risk of scoliosis(15), and sport does not harm scoliosis in general(16). Rather, sport, dance and physical games promote dexterity, the ability to balance and general body awareness. They help therapies such as the Schroth Method or manual therapies such as osteopathy or Rolfing to work better. Climbing, bouldering, slacklining (balancing), swimming, horse riding, dancing, ballet, athletics, floor gymnastics and Pilates are beneficial sports. Avoid weightlifting, high diving, golf, tennis, gymnastics or bodybuilding. Strength training is also the wrong approach because you cannot train scoliosis away by building up individual muscles. Rather, it is a matter of learning a new movement pattern by activating muscle chains – which preferably extend from head to toe – and integrating them into your everyday life and into your sport so that this movement becomes a second nature.
Balance exercises
Propriozeption is the sense for the position of your body in space and, together with the sensitivity to depth and the sense of balance, helps people to straighten up, to move, to walk and also to balance. Scoliosis patients have deficits here because the internal map of their body, represented in the brain, is partially distorted or not sufficiently pronounced(17). This causes scoliosis patients to move crookedly, but believe that they are straight. Here, balance exercises, preferably performed in front of the mirror, can help to align this internal proprioceptive map with reality. Therefore, balance exercises should be used with every scoliosis therapy. Frequent balancing strengthens the new pathways in the brain. In this way, movement patterns can change, the body learns to behave stably and at the same time elastically in an unsafe situation, and posture is improved. In the past, this was done by putting a book on the head of a young girl or by letting her walk on a rope. In my practice I like to use the Tuning Board by Darrell Sanchez.
Somatic Experiencing SE
The Somatic Experiencing® method deals among other things with disturbances in the nervous system, which can also affect the sense of balance. These disorders may have arisen in early childhood or may be caused by traumatic events. In SE therapy, the autonomous nervous system is induced to reorient itself, which can also resolve balance disorders. These are closely linked to the orientation reaction, the basis from which the brain projects a movement and then executes it. The SE method will not eliminate scoliosis, but it can help you find a safe base.
Chiropractic
The American Chiropractic is an independent profession in the USA, which may even do surgery in some states. For the treatment of scoliosis, local chiropractors like to market a combination of chiropractic, Schroth method and SpineCore corset. Marketing strategies and the ethics of the profession are under discussion in the USA(18). American Chiropractic is rarely found in Germany. Here in Germany, chiropractic may be practiced by a doctor or alternative practitioner with appropriate additional training. From my point of view it can be used for very severe scolioses in addition to manual therapy such as Rolfing or osteopathy.
Osteopathy
In the Anglo-American countries and in Europe, osteopathy is a recognized profession with extensive training. Recently there has been an increasing effort to prove the effectiveness of the method through studies, which has been partially successful. Osteopathy is certainly a good choice for the treatment of scoliosis in children in their early stages. It is also suitable for the treatment of functional disorders caused by scoliosis in the organs and fine membranes of the brain. Osteopathy is a self-contained medical system that follows the principles of applied anatomy, physiology and pathology. It is based on the assumption that the body is a unit which always participates as a whole in health and illness.
Rolfing
Rolfing® – Structural Integration has recently been associated more frequently with findings from fascia research by Robert Schleip(19) (20)..The properties of fascia are redefined by this research; these findings are noticed in the fitness and sports community and are discussed at congresses(21). In Rolfing one works with the fascial structures in the body in order to release chronic tensions and thus enable the body to stand up and move freely. Rolfing is therefore ideal for the treatment of scoliosis. Each scoliosis is a slow movement, in which the body twists and contracts at the same time, so that the spine moves sideways. The entire fascial system from the head to the spine to the feet is affected by this scoliotic twisting. In Rolfing, we work to unwind this scoliotic torsion, i.e. to achieve de-rotation and de-compression of the spine. – There are impressive case studies of what the Rolfing method can achieve.
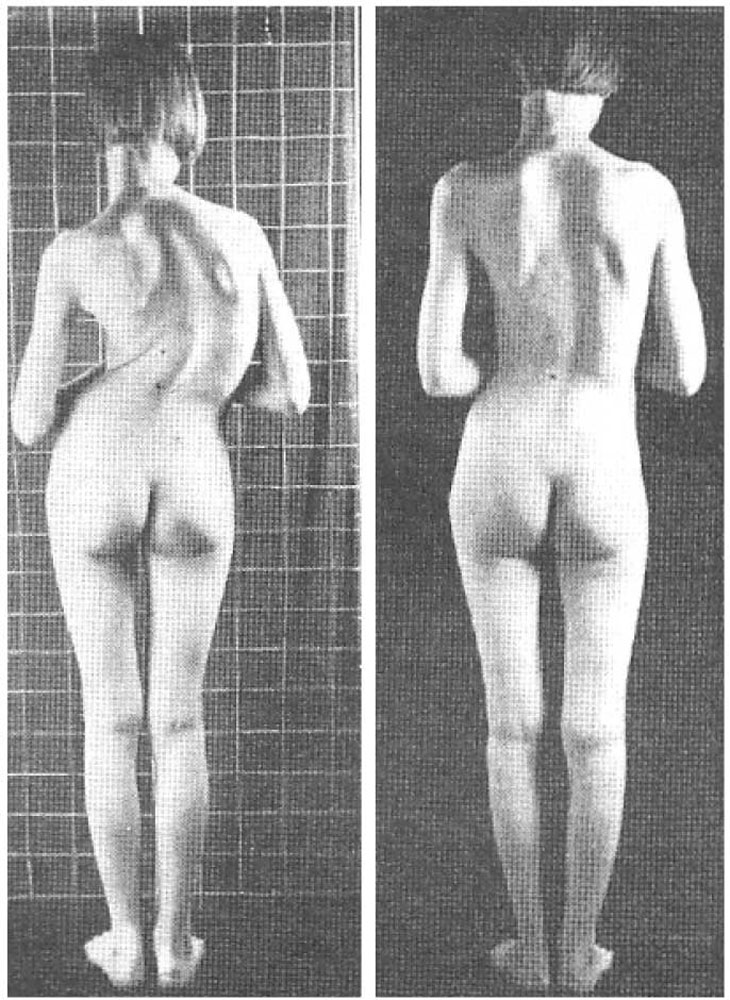
Erik Dalton describes in “Scoliosis: A Case Study” how he treated the pictured girl with the Rolfing method in 1993. The two photos are 3 years apart(22).
Dynamic corsets
An alternative to the hard shell corset is the dynamically correcting corset from SpineCore. It allows the body the necessary freedom of movement, can be worn under clothing and is used for children and adults up to an angle of approx. 30° on the Cobb scale/angle. Actually, it is not a corset, but rather a kind of bandage that gently pushes the body into the new movement pattern. However, the SpineCore corsets are not suitable for every scoliosis, they demand skill and expertise from the orthopaedic technician and committed behaviour from the patient. Currently, SpineCore corsets are only available in Freiburg, Germany.
Hard shell corsets
I do not share the view that one waits and does nothing until the scoliosis has reached 20° and then prescribes a corset. Rather, even low-grade scolioses should be treated as early as possible. Hard shell corsets are always controversially discussed. They reduce the quality of life(23), and reduce the vital capacity of the lungs because they compress the ribs(24). The reduced lung function is comparable to that of a smoker. Corsets restrict movement, which is why the back and abdominal muscles atrophy (shrink); in the long term, joint problems can arise due to the lack of movement. The corset impedes mobility at a time when young people should try out their bodies intensively and move around a lot. If the corset is taken off, the body tends back to the scoliotic pattern because it could not create a new movement pattern. Therefore, it must be “trained out”, i.e. slowly discarded. Behind the corset is the idea that scoliosis can be pushed out of the spine laterally. This is a mechanical rather than a neurological view. If the back is slightly crooked and the brain thinks it is straight, movement therapy makes more sense than immobilization through a corset. Nevertheless, corsets continue to be prescribed because they have proven their worth to a certain extent. The corset technique has been refined in recent decades, but the success rate between corset types is very different(25). Unfortunately, it is impossible to predict whether and to what extent scoliosis will worsen. According to a study, 72 % of corsets are therefore successful depending on how long they are worn, compared to 48 % in the control group, which did not experience any deterioration without the corset. In other words, corsets are largely unnecessary, but one does not know when(26),(27). In summary, if scoliosis becomes increasingly severe despite the use of alternative therapies and all your efforts, the corset may become necessary.
Operation
Orthodox medicine recommends surgery from a 40° Cobb angle. During the operation, metal rods are inserted and spinal sections are stiffened. The rate of complications caused by the operation is considered high(28). 19 % of those who have undergone surgery must be post-operated(28). 10 % have postoperative pain for more than one year(29). 25 % of those who have undergone surgery have chronic pain and therefore visit a pain clinic after years(29). 15 % of children report moderate to severe pain five years after surgery(30). Adolescents say they have more pain five years after surgery compared to two years after surgery(31). The failure rate of spinal surgery is assessed very differently and it seems difficult to predict failure based on factors such as tobacco use, obesity, depression, social factors or stress(32). The decision for or against surgery is also discussed among experts and examined in metastudies(25),(33) worth reading. The list of pros & contras from kidhealth.com(34) is clear and understandable for the average person. – The decision is certainly not easy and always depends on the individual case. If you have decided to have an operation, you need a surgical team that will advise you well and also look after you after the operation.
Graphic: Scoliosis Syndrome By Karena Thek
My recommendation
You will not need or be able to take advantage of all the above therapy options. Therefore here now my recommendation.
- Medical specialist:
Please visit follow-up checks regularly please clarify sensorimotor insoles Bite correction by the orthodontist - Physiotherapy:
Spiraldynamik, Schroth-Method, preferably from one source with the physiotherapist – so that you can get into motion and get to know your movement patterns. - Sports
At least 3 times per week e.g. climbing, jogging, swimming, water aerobics, etc. - Manual therapy:
Rolfing or osteopathy or both – so that the chronic tensions in the muscles and fasciae are gradually released. - Movement training:
You need a coach for movement, posture and for your self-perception of standing upright. This can be a Feldenkreis teacher, dance teacher or Pilates trainer. - Balance exercises
You should balance daily for a few minutes. It helps you build stability and trains the nervous system. I have listed it as an extra point because this exercise is so essential.
My way of working
In my practice we will find exercises specially tailored to your needs that you can integrate into your everyday life. We will work on your posture, your gait and the way you sit on chairs. We look at those movements your body lacks, has forgotten or doesn’t know, and then explore new movement possibilities. We explore how you can create stability and length in your body. It is not about control that you force on your body, but rather about playful searching, trying out and exploring new territory.
I will pave the way to this new, stable and yet flexible posture by releasing hindering tensions in your body with the Rolfing method. For this purpose you will spend more than half of the time on the massage bench in each session.
But much more important is that you become active in your everyday life, that you try again and again to deal consciously with your body and that you find joy in creative play with movement, that you are active in sports or dance and develop a feeling for balance.
This is the way I can accompany you or your child.
Journal Rückenzeit
In the journal „Rückenzeit“ you will find an interview with Stephan Lautz about scoliosis. Just click on the picture or here.

References:
1 Quelle Foto: www.kid-check.de Die Aktion gegen Haltungsschwäche!
2 “SOSORT 2012 consensus paper: reducing x-ray exposure in pediatric patients with scoliosis” Patrick Knott, Eden Pappo, published 2012
3 “2011 SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth” Stefano Negrini, published 2011
4 Davissches Gesetz Wikipedia
5 “Development of Auditory and Vestibular Systems” Book by R. Roman Seite 501
6 “Horizontal postrotatory nystagmus response in female subjects with adolescent idiopathic scoliosis” Jensen GM, published 1979
7 “Vestibular Asymmetry as the Cause of Idiopathic Scoliosis: A Possible Answer from Xenopus” François M. Lambert, published 2009
8 “Does adolescent idiopathic scoliosis relate to vestibular disorders? A systematic review.” Catanzariti JF published 2014
9 “Hypothesis on the Pathogenesis of Idiopathic Scoliosis” F.H: Wapstra , published 2012
10 “Wechselwirkungen zwischen Körper- und Kieferasymmetrie? Untertitel: Bedeutung der pädiatrischen Vorsorgeuntersuchung mit kieferorthopädisch-orthopädischem Screening” Heike Korbmacher, Dr. med dent, Gerald Eggers-Stroeder
11 “Sensomotorische Einlagen: Bei Beschwerden können sie helfen?” BR Fernsehen
12 www.fussgesundheit.info
13 “Effektivität und Wirksamkeit einer funktionell-dynamischen Schuheinlagenversorgung im Sport” Heiner Baur, Dissertation 2004, S. 119 ff
14 “Probleme mit Hatha-Yoga-Übungen bei Skoliose”von Christa Lehnert-Schroth, ca 2014
15 “Physical activities of Patients with adolescent idiopathic scoliosis (AIS): preliminary longitudinal case–control study historical evaluation of possible risk factors” Marianne E McMaster, published 2015
16 “Is physical activity contraindicated for individuals with scoliosis? A sytematic literature review” Bart N. Green, published 2008
17 “Scoliosis and Proprioception” by Robert Schleip published 2000
18 “Chiropractic controversy and criticism” Wikipedia
19 www.somatics.de Webseite von Dr. Robert Schleip
20 Deutsche Gesellschaft für Myofascial Release e.V.
21 Fascia Research Congress
22 “Scoliosis: A Case Study” Eric Dalton, ca 1993
23 “Outcome assessment of bracing in adolescent idiopathic scoliosis by the use of the SRS-22 questionnaire” Kenneth M.C. Cheung, 2006
24 “Pulmonary restrictive effect of bracing in mild idiopathic scoliosis” J D Kennedy, published 1987
25 “2011 SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth” Stefano Negrini, published 2011
26 “Auswirkungen einer Korsettversorgung bei Jugendlichen mit einer idiopathischen Skoliose: die BRAIST – Studie” Carolin Reuschel
27 “Effects of Bracing in Adolescents with Idiopathic Scoliosis” Stuart L. Weinstein, published 2013
28 “Rate of complications in scoliosis surgery – a systematic review of the Pub Med literature” Hans-Rudolf Weiss, published 2008
29 “Persistent pain in patients following scoliosis surgery” G. T. C. Wong, V. M. Y. Yuen, published 2007
30 “Pain prevalence and trajectories following pediatric spinal fusion surgery.” Sieberg CB, published 2013
31 “Adolescent idiopathic scoliosis patients report increased pain at five years compared with two years after surgical treatment.” Upasani VV, published 2008
32 “Predictors of surgical outcome and their assessment” Anne F. Mannion, published 2006
33 “Adolescent idiopathic scoliosis – to operate or not? A debate article” Hans-Rudolf Weiss, published 2008
34 “Cons of Having or Not Having Surgery” and “Pros of Having or Not Having Surgery” by www.aboutkidshealth.ca
35 Quelle Foto: Muscle Imbalances and Scoliosis
If you have any questions, please feel free to contact me in my practice in Berlin or Munich. Here you will find the contact page.